This post examines the regional campus component of needs based funding, which starts this year. I looked at the low SES and Indigenous component last week.
The regional component funds students at regional campuses rather than regional students. It assumes higher average costs at regional campuses. A longstanding ‘regional loading’ served a similar purpose. Just under $90 million was spent on the regional loading in 2025. Universities have been notified of their needs based funding amounts, but as of 23 February 2026 I cannot find a public record of them.
The research on cost by campus
The Deloitte Access Economics costing work used by the Morrison government to reset funding rates found that regional universities had higher costs per EFTSL after controlling for other factors affecting costs, such as discipline.
Later work by the U of M’s Centre for the Study of Higher Education, using Pilbara Group data, also found that regional campuses had higher average costs per EFTSL (chart below). This partly reflects a general feature of university costs – higher education is an economies of scale enterprise, but regional campuses on average have lower enrolments than major city campuses. However, higher regional costs were found to be still present after controlling for subject size.
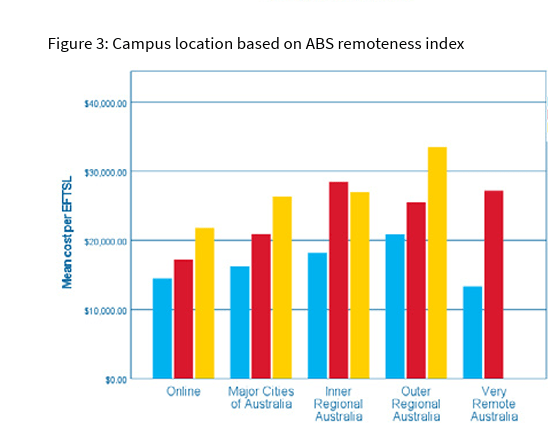
Assuming that higher education should, ideally, be taken to where the students are – a proposition I agree with – the basic policy idea behind the regional loading/regional component of needs based funding is sound.
Read More »